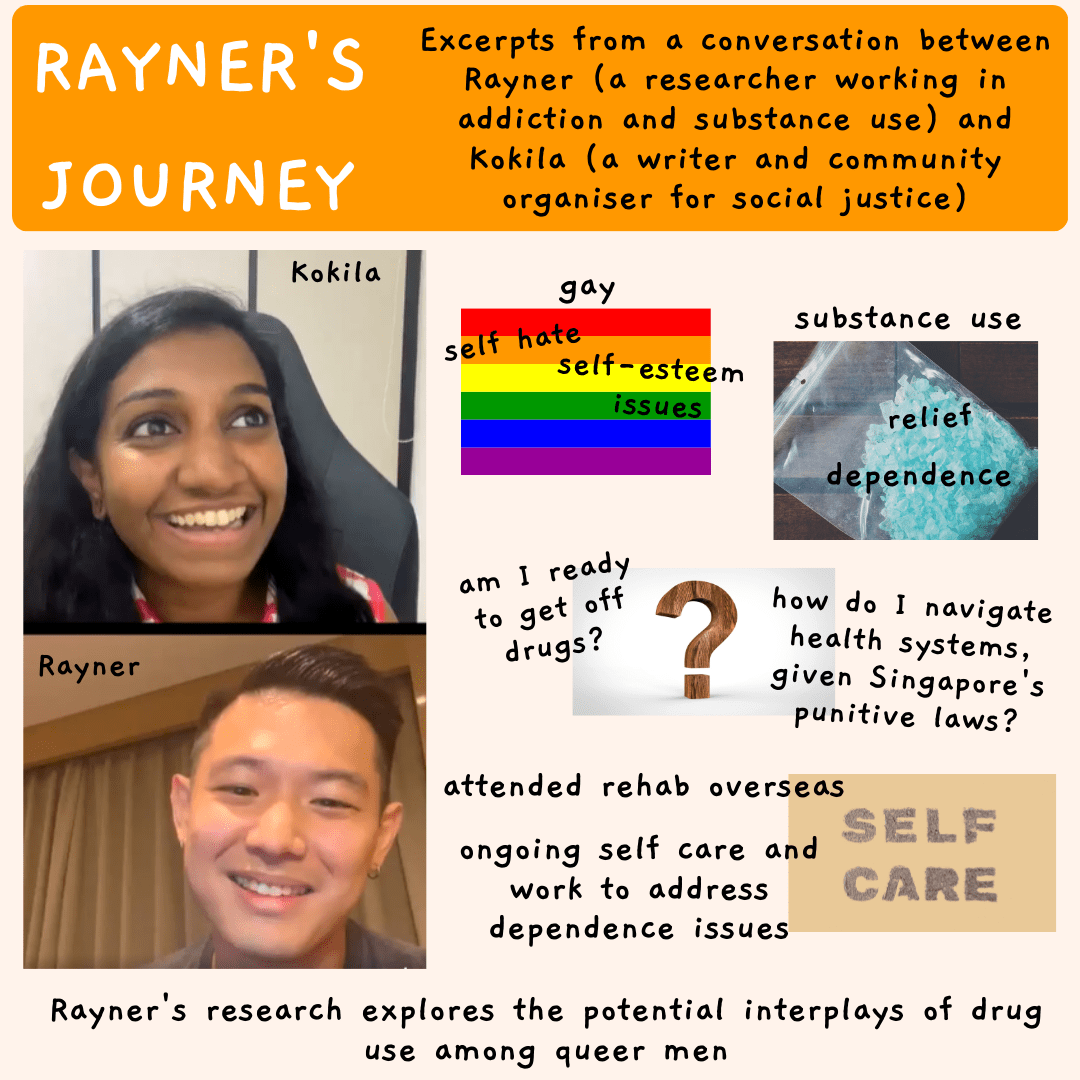
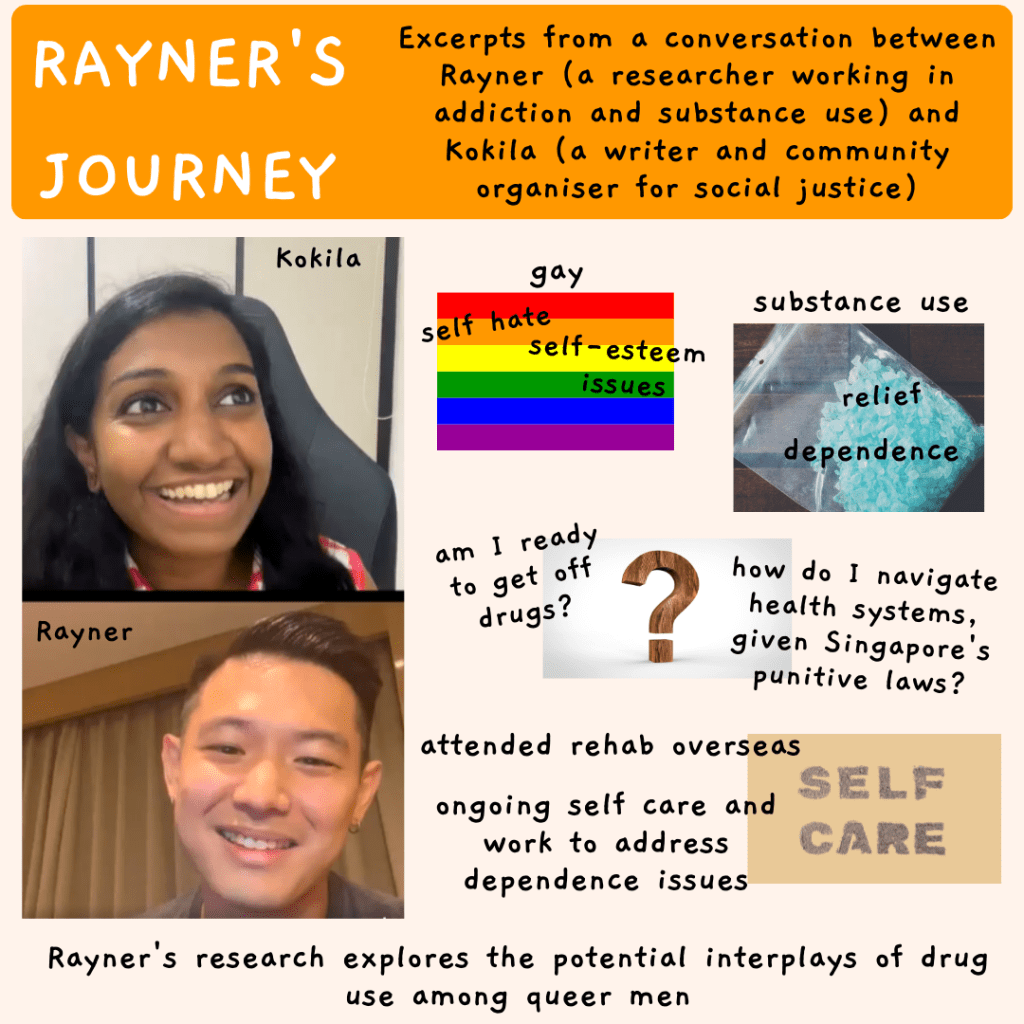
TJC’s Drug Policy working group is underpinned by understanding and supporting harm reduction, enacted through community building, consultations with drug users, community conversations and more. In this discussion streamed on Instagram Live, Rayner (a researcher working in addiction and substance use) and Kokila (a writer and community organiser for social justice) discuss Rayner’s story.

Rayner’s journey
When Rayner was first introduced to substances, there seemed to finally be a way to stem the self-hate and self-esteem issues placed upon him, navigating the world as a gay man. The relief provided by substance use, particularly crystal meth, escalated into dependence after a series of traumatic events including physical assault. Although Rayner’s family and friends attempted interventions, Rayner was in a space where he was incapable and afraid of getting off drugs. Even when ready at times to explore rehab, he was unsure of how to navigate health systems in the context of Singapore’s punitive laws. Rayner attended rehabilitation overseas, and is now doing ongoing self care and work to address dependence issues. His own experiences drive his research work, which explores the potential interplays of drug use among queer men.
Health systems, equitable care and harm reduction
Rayner’s story highlights societally restricted, implicit yet unasked ponderings. What is the purpose of health and healthcare? What factors are at play which enable or restrict access to health? What does health equity and access look like in terms of substance use? Health is a state of complete physical, mental and social wellbeing — necessitating health rights and equity, not just about presence of disease. This is a languaging which tends to be absent in Singapore’s health system, which focuses heavily on substance use as criminal rather than from a wellbeing-focused lens. Harm reduction is also a helpful way to understand more humane and effective approaches to substance use, and is aligned with aspects of health and wellbeing. It is a liberating framework which respects autonomy, facilitates boundary-setting and protecting, while increasing safety and wellbeing, and is context-specific in catering to specific needs and support.
Substance use in itself is not a disorder, but unhealthy dependence can be. Many of us imbibe substances in daily life — coffee, alcohol, nicotine and more, and knowing our relationships with substances, whether illicit or not, whether healthy or not, whether fuelling our wellbeing or not, is key. Individuals would be able assess these and discover what works for them individually through education around substance use — access to resources (e.g. institutions which can provide information), a mix of local and international research (the former of which is sorely lacking), and trauma-informed approaches. We know that it is not about simply removing drugs from people — there are complex underlyings and a mix of approaches grounded in harm reduction, drug demand reduction and rehabilitation serve the individual much more effectively than criminalisation. We also need to recognise that for those involved with drugs, substances are looked at as a solution rather than a problem — a narrative that is well-established in recovery rooms and rehabilitation. Understanding how and why people use substances should be the starting point, rather than coercing people to stop use. Substance use has been looked at in binaries, and therefore been oversimplified, resulting in simple ‘solutions’ to complex issues.
Equitable systems center those who need the support and care. Singapore’s current system ensures those apart from the people involved with drugs are made to think they need protection from those who are involved with drugs. In this way, the system creates an ‘us’ and ‘them’ mindset which could be incorrectly in-grouped as those who use and those who don’t, rather than those who need and want community. Policies tend to neglect people who are actually involved with substances, by pedestalising those who are not involved with drugs.This also calls into question how health systems are not fulfilling obligations as part of their commitment.
Criminal or moral perspectives, including history of drug politicisation
In understanding one’s own relationship with substances, a harsh narrative of ‘don’t use’ prevents someone from actually navigating help and support on their own terms, through better understanding of how to moderate or stop their use. In Rayner’s experiences, given the framework of systems he operates in, it would be unethical for him to say anything else but “stop using”, or “don’t tell me you’re using substances”. This closes off pathways to wellbeing and empowerment for the individuals who are using substances, wherever on the spectrum they are — be it in addiction, wellbeing, understanding, or regulation. The resulting stigma and fear (e.g. of incarceration) contribute as key barriers to health access. The criminal or moral perspective is incongruent with health perspectives, and highlights the underlying political decision-making in denying health equity in substance use.
Criminalisation causes harm, and decriminalisation of use and possession, and legalising and regulating sales is a big part of harm reduction. According to Harm Reduction International, statistical findings from countries that have reduced or abolished criminal penalties for drug possession underscore three important findings, namely that the rate of drug use or crime did not increase; the rate of addiction, overdoses, and HIV/AIDS sharply decreased; and more people entered drug treatment programs. What actually harms those involved with drugs are the punitive laws, the trauma of incarceration, the ordeal of CNB raids, the fear of getting caught, the extreme disruption to their lives caused by incarceration, urine testing, probation, supervision regimes, and other aspects infused so heavily into the criminalisation of drug use. One of the most troubling realities is that doctors are actively disabled and disempowered from truly helping and providing health support for people who are experiencing substance use or dependence. Doctors are mandated to report any signs of drug use, and both them and their patients are disallowed from freely discussing the patient’s health needs. Even doctors who apply their medical expertise and try to offer those who experience dependence less harmful substances to use or utilise other harm-reduction practices get criminalised.
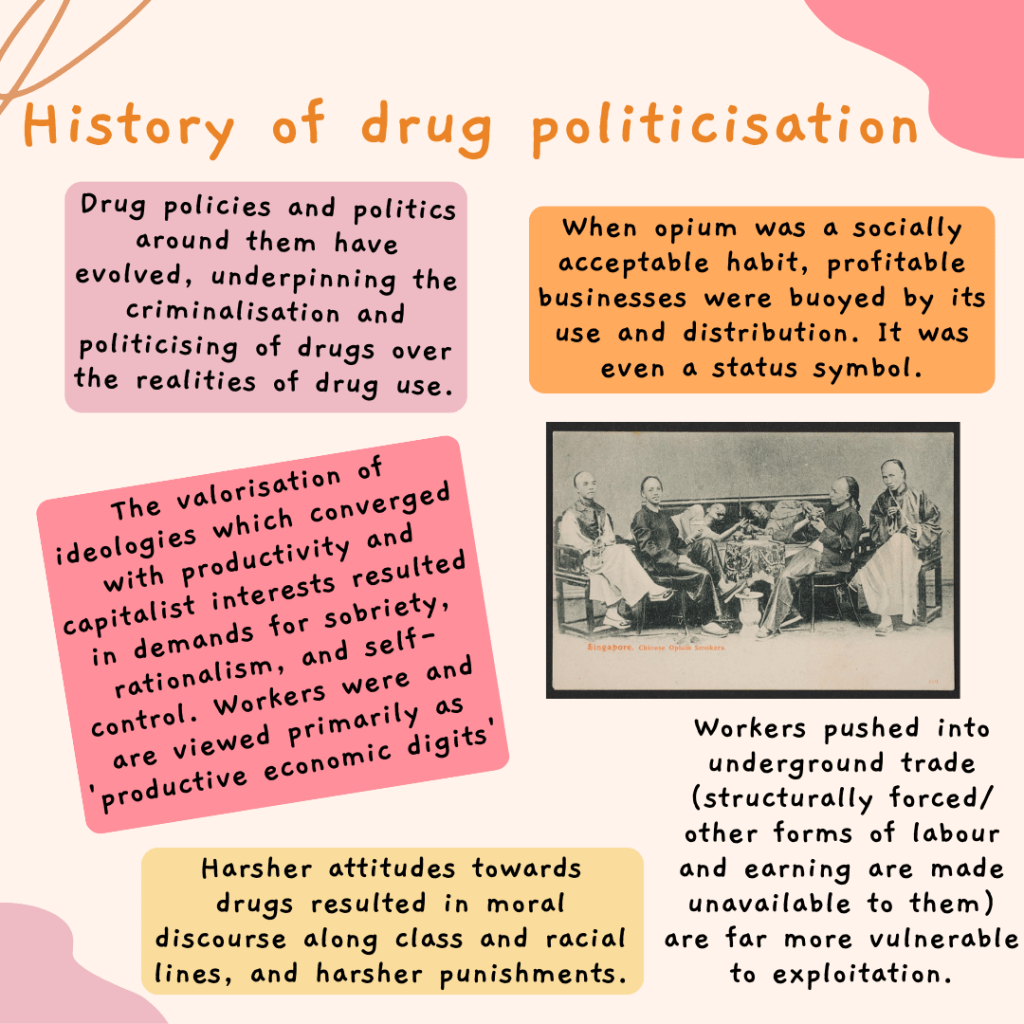
It is also necessary to understand the evolution of drug policies and politics around them, which underpins the criminalisation of drugs and politicising of drugs over the realities of drug use. Back when opium was a socially acceptable habit, profitable businesses were buoyed by its use and distribution, and it was even a status symbol. Following Singapore’s independence, which was undergirded by neoliberalism, the valorisation of ideologies which converged with productivity and capitalist interests resulted in demands for sobriety, rationalism, and self-control. Workers were viewed primarily as ‘productive economic digits’. This created the need for harsher attitudes towards drugs, and a resulting moral discourse along class and racial lines (e.g., ‘ghettoising’ behaviour). Higher rates of relapse and recidivism led to harsher and harsher punishments. Creation of the misuse of drugs act, zero tolerance policy, Singapore’s mirroring of the UN narcotic drugs policy, and the unscientific classification and reclassification of different drugs all worked hand in hand to concretise the criminalisation of drugs.
Exploitation and reorienting views of those in drug trade
When an industry is pushed so heavily underground through extreme forms of criminalisation, whether sex trade or the drug trade, workers in it are far more vulnerable to exploitation. There are those who are structurally or otherwise forced into these trades as the primary or even sole form of earning. There are those who may not be able to access help for their dependence, given the heavily punitive and disruptive system, and may stay dependent and forced into low-level sales as a way to sustain their dependence. There are those for whom other avenues of labour are made unavailable to them. All these workers have little formalised or even informal modes of protection, and acquiesce to the risks of facing capital charges. As more and more desperate people who have no real choices end up participating in the trade, abusive practices increase as individuals in the trade become expendable and replaceable. If we reorient our view of ‘drug traffickers’ to ‘drug trade workers’, we move the conversation to an economic-based one which centers providing for self and family. By recognising the funnelling of workers into this industry, we can have real conversations about the exploitation that happens to those forced into the work. Even those who may not be forced into the industry are still exploited through the very nature of it being criminalised.
Death penalty and future research
Despite the strong ‘drug-free country’ narratives that Singapore espouses, there has been insufficient research on drugs and the people involved with them. The state has made claims around the effectiveness of the death penalty in reducing inflow of substances, but it is weak evidence with feigned causal relationships, therefore the claims are not robust. Are these rhetorics grounded in sound research or are they fashioned to create moral panic? Given that the environment is aggressive with wide-reaching government propaganda, and with little data transparency, research on attitudes and other aspects related to drugs is much more fraught and far less instructive. There is also restricted media freedom or freedom of information in general, thus knowledge dissemination methods are not made, nor are made accessible.
There are three huge considerations for policy-focused research at a population level. Firstly, we need more research which explores wellbeing — beneficial, recreational, self-regulated substance use, substance dependence and addiction. And together with this we need to better understand access to care, importantly including intersectional approaches around race, socioeconomic status, sexual orientation and disparities in access. Secondly, there has to be better understanding of social attitudes and changes in policies, and such research should be supported by the state (such as other studies done about what are viewed as socially divisive issues). Thirdly, we should explore, at the existential level, what our capital punishment with regard to drug policy is supposed to achieve and, even if it is defined, we should ask whether we are achieving it in an equitable way.
It is important to continue asking questions — questions which have not been addressed, and which we should not be afraid of addressing. What is the reality and the effect of the death penalty regime for drugs? How are the lines blurred between users and workers in the drug trade? How does the death penalty for couriers impact people experiencing dependence/ addiction? Can the state take life? Can we give the state the right to take life? It is also important to have more conversations, and amongst those who have stakes in the issues, and recognise that we can and should be making demands. We can demand reduction – harm reduction and decriminalisation. We need evidence-based policies. We need to ask how we can support people’s bodily autonomy while minimising harm. We need to question how to destigmatise pleasure, and how to alleviate pain. We need to have deeper, constructive, understanding conversations between people involved with drugs, policymakers, scientists, researchers, and abolitionists. And these conversations should be grounded in recognising and owning that we are experts of our own lives and we all have a right to self-determination. We have autonomy and agency, and do not have to be subject to authority power simply out of fear or coercion. Conversations could be open, including navigating wellbeing even in the absence of decriminalisation or abolition. In the mean time, we could try and be/become a trusted person that people in our lives can turn to if they need support, for substance use or otherwise. And to think about what it would look like to support people who are struggling with dependence in ways that keeps them safe from harmful and punitive state intervention.
Watch a recording of the IG Live here:
